Non-Operative Management of UCL Injuries
When a pitcher feels pain on the inside of the elbow and hears the words “UCL injury,” the immediate assumption is often Tommy John surgery.
In reality, that’s not always the best first step.
A large percentage of UCL injuries in throwers are partial tears or ligament sprains, not complete ruptures. With the right management strategy—rest, targeted strength training, and a structured return-to-throwing program—many athletes can return to high-level throwing without surgery.
The key is understanding what actually happened to the ligament and how to rebuild the system around it so the elbow isn’t forced to absorb more stress than it can tolerate.
What the UCL Actually Does
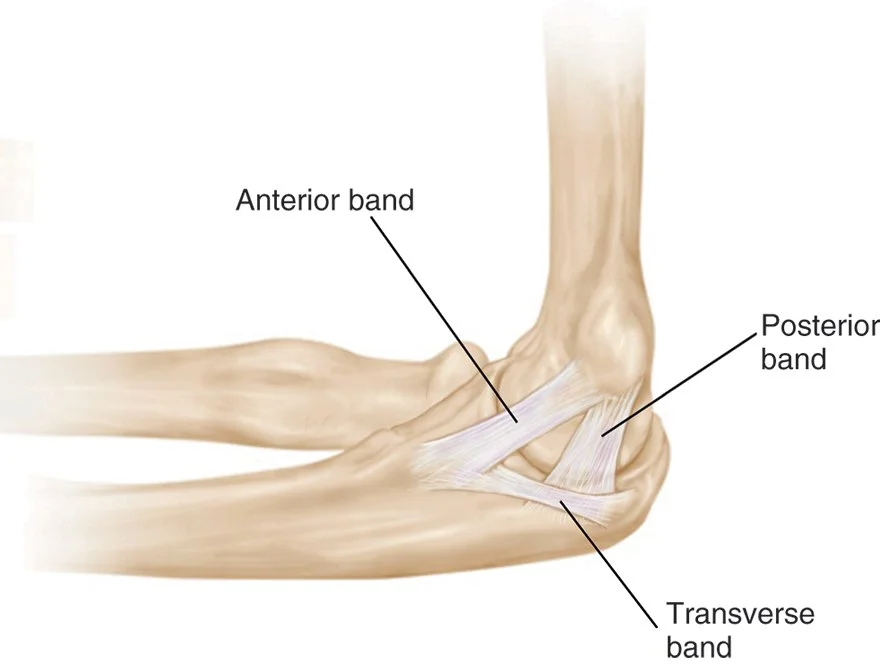
The ulnar collateral ligament (UCL) is the primary stabilizer on the inside of the elbow that resists valgus stress.
Valgus stress is the force that tries to bend the elbow inward during the throwing motion.
At ball release, the elbow experiences extremely high forces, often approaching or exceeding the structural limits of the ligament. The UCL works with surrounding muscles to prevent the elbow from “opening up.”
Those supporting structures include:
Flexor-pronator mass (forearm muscles that dynamically stabilize the elbow)
Rotator cuff (controls humeral head positioning)
Scapular stabilizers (allow efficient energy transfer from the trunk)
When the kinematic sequence—the coordinated transfer of energy from the legs → trunk → arm—is disrupted, the elbow often becomes the structure that absorbs the extra stress.
In simple terms:
If the body stops transferring energy efficiently, the elbow pays the price.
How UCL Injuries Actually Occur
Contrary to popular belief, most UCL injuries are not a single catastrophic event.
They are usually the result of repetitive microtrauma from thousands of throws.
Common contributors include:
Excessive throwing volume
Poor arm recovery between outings
Velocity spikes without adequate strength development
Loss of overhead mobility or total rotational mobility at the shoulder
Poor scapular control
Over time, the ligament begins to lose its ability to tolerate stress.
Grading UCL Injuries
Grade 1
Mild stretching of the ligament fibers
Pain with throwing but ligament integrity largely intact
Grade 2
Some ligament fibers are disrupted
Stability may still be preserved
High-Grade Partial Tear
Significant fiber disruption
Complete Tear
Full rupture of the ligament
Typically requires surgical reconstruction
The location of the tear also matters.
Research shows that proximal tears (closer to the humerus) often respond better to non-operative treatment than distal tears.
When Non-Operative Treatment Makes Sense
Current sports medicine literature supports non-operative management as the first line of treatment for many UCL injuries, particularly:
Low-grade tears
Proximal ligament injuries
Timeframe where surgery doesn’t make sense (high school/college senior)
Studies examining structured rehab programs have reported return-to-play rates between roughly 40–90% depending on tear severity and athlete level. That essentially means we really don’t know if someone is going to successfully complete a non-op approach, but if the clinical signs add up, it is worth a shot.
Successful rehab programs focus on restoring the entire throwing system, not just the elbow.
Phase 1: Protect and Calm the Elbow
Goals:
Reduce irritation to the ligament
Restore pain-free motion
Common interventions:
Temporary shutdown from throwing
Soft tissue work to the forearm, elbow, and posterior cuff to restore mobility
Begin improving forearm and shoulder strength if tolerable
Red Flag:
If elbow pain occurs with daily activities or simple gripping, the elbow is not ready for loading.
Phase 2 (blend into phase 1 if tolerable): Build the Dynamic Stabilizers
The elbow relies heavily on muscle support during throwing.
Key areas to strengthen:
Flexor-pronator mass
Rotator cuff
Scapular stabilizers
Examples of exercises:
Forearm
Wrist flexion/extension
Pronation/supination
Rotator Cuff Loading
External rotation
Standing full can
Scapular Control
Prone Y/T
Serratus wall slides
The goal is to create muscular support that reduces stress on the ligament.
Phase 3: Restore Power and Arm Speed
Before returning to throwing, the arm must tolerate high-speed loading.
This is where many rehabs fall short.
Athletes should progress to:
Med ball rotational throws
Plyometric cuff training
These exercises restore the explosive arm action required for pitching while ensuring the elbow can tolerate the forces involved.
Phase 4: Structured Return to Throwing
Throwing should never be random during rehab.
A structured progression typically moves through:
Short distance catch play
Gradual distance increases
Controlled mound work
Full intensity pitching
Each step should only progress if the athlete remains:
Pain-free
Maintaining velocity and command
Recovering normally between throwing sessions
The Bottom Line
Not every UCL injury requires surgery.
Many throwers with partial tears can successfully return to play with a well-structured rehabilitation program.
Effective non-operative management focuses on three priorities:
Reducing stress on the ligament to allow it to calm down
Strengthening the muscles that support the elbow
Proper ramp up
If the athlete can restore strength, mechanics, and workload tolerance, the elbow often becomes symptom-free and resilient enough to handle high-level throwing again.
Unfortunately, many athletes who attempt non-operative treatment will ultimately require surgery. The stresses placed on the elbow during high-level throwing are enormous, and in some cases the ligament simply cannot tolerate those forces long-term.
However, following a structured, evidence-based rehabilitation plan gives athletes the best possible chance to succeed without surgery. Even for those who eventually require reconstruction, this process builds the strength, mobility, and movement quality that are essential for a successful surgical outcome and smoother return to play.
The biggest mistake athletes make is trying to throw through pain or rushing back before the arm is prepared to tolerate the stress of pitching.
When rehab is done correctly, the goal isn’t just getting back on the mound.
It’s returning with an arm that is stronger, more efficient, and better prepared for the demands of the season.